


Migration Coding in Primary Care From 2011 to 2025 Using the New OpenCodeCounts Tool
- Posted:
- Written by:
- Categories:
Migrants, defined here as people born outside of the UK, represent a significant proportion of England’s population at 17.4% or 9.8 million individuals. The conditions that a person lived in before migrating, their migration journey and then living in a country as a migrant can all affect their health. For this reason, it’s important that we understand migrants’ health needs so that we can identify any health inequities and take the appropriate action to address them.
Everyone in England is legally entitled to access and use primary care free of charge, regardless of their immigration status. Migrants often face barriers to accessing care. For individuals who do manage to access primary care, the recording of their migration status is not compulsory in the electronic health records (EHRs). However, it is still sometimes recorded in the form of SNOMED CT clinical codes, which are numbers combined with descriptions (e.g. “ Asylum seeker awaiting decision on refugee status” - 728611000000100) or in the form of free text (e.g. “patient is a refugee”). In this study, we wanted to better understand the recording of migration status using SNOMED CT codes in English primary care.
To do this, we compiled lists of SNOMED CT codes that relate to migration (for example, “refugee” or “interpreter needed”) and then looked at how often these were used in primary care. We did this using our new tool, OpenCodeCounts, which allows users to explore primary and secondary care coding trends interactively (using the web tool) or programmatically (using the R package). It is underpinned by publicly available data published by NHS England on annual SNOMED CT code usage in primary care and hospital activity from 1st August 2011 to 31st July 2025.
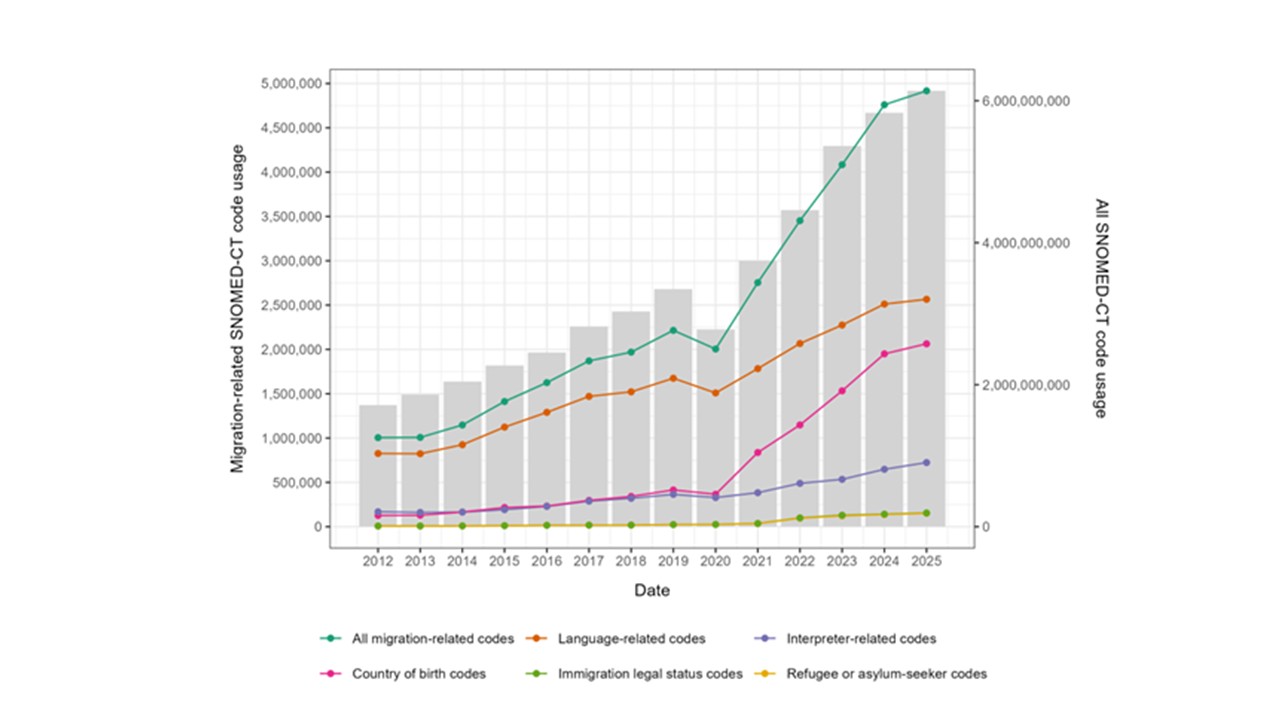
We created the following different lists of SNOMED CT codes and looked at how often these lists of codes are used over the study period:
- All migration-related codes
- Country of birth codes
- Immigration legal status codes
- Asylum or refugee status codes (a subset of immigration legal status codes)
- Language-related codes
- Interpreter codes (a subset of language codes)
What did we find?
- 1,119 codes related to any aspect of migration (e.g. country of birth, language and legal statuses) were used a combined total of 34.2 million times from 2011 to 2025
- Migration-related coding has increased over time, particularly from 2020 and in the case of country of birth and language codes
- Language was the most commonly recorded characteristic
- The coding of immigration legal statuses was low and dominated by asylum and refugee codes
What do these findings mean?
That it is feasible to use SNOMED CT migration codes in EHRs to create cohorts of migrants
In order to create cohorts of migrants in primary care, we look for a migration-related code in their EHR. If they have such a code, we add the individual to our cohort. Through showing that there were over 34 million uses of migration-related codes, we demonstrate that migration coding is common enough to likely allow us to create a cohort of migrants.
That the migrant cohorts that we create may be biased towards people with a previous or current English language barrier
Our analysis showed that language codes were the most commonly used, which suggests that people who have an English language barrier may be more likely to have code added to their EHR. This is important to keep in mind when doing future research with the migrant cohort, because we may not be capturing all types of migrants (e.g. individuals who come from English-speaking countries, or who arrive with a high level of English proficiency) and therefore, the results would not reflect the health needs of all migrants.
What’s next?
This study demonstrates that SNOMED CT codes can be used to create cohorts of migrants in primary care data and is part of a wider project on exploring migrants’ health in EHR data, which is part of a Bennett Junior research fellowship. Next, subject to a successful application, we plan to apply these SNOMED CT code lists to primary care data in the OpenSAFELY platform in order to conduct studies to understand migrants’ health needs.
Please read the paper for the full results and our suggestions for future work in this area.